|
|
|
|
|
US
|
3,500
|
36.2
|
|
Germany
|
1,097
|
11.4
|
|
Japan
|
1,000
|
10.4
|
|
UK
|
733
|
7.6
|
|
European Commission
|
489
|
5.1
|
|
Italy
|
470
|
4.9
|
|
Canada
|
384
|
4.0
|
|
Sweden
|
296
|
3.1
|
|
France
|
244
|
2.5
|
|
Gates Foundation
|
206
|
2.1
|
|
Saudi Arabia
|
153
|
1.6
|
|
Norway
|
141
|
1.5
|
|
Subtotal
|
8,713
|
90.2
|
|
Grand total
|
9,661
|
100.0
|
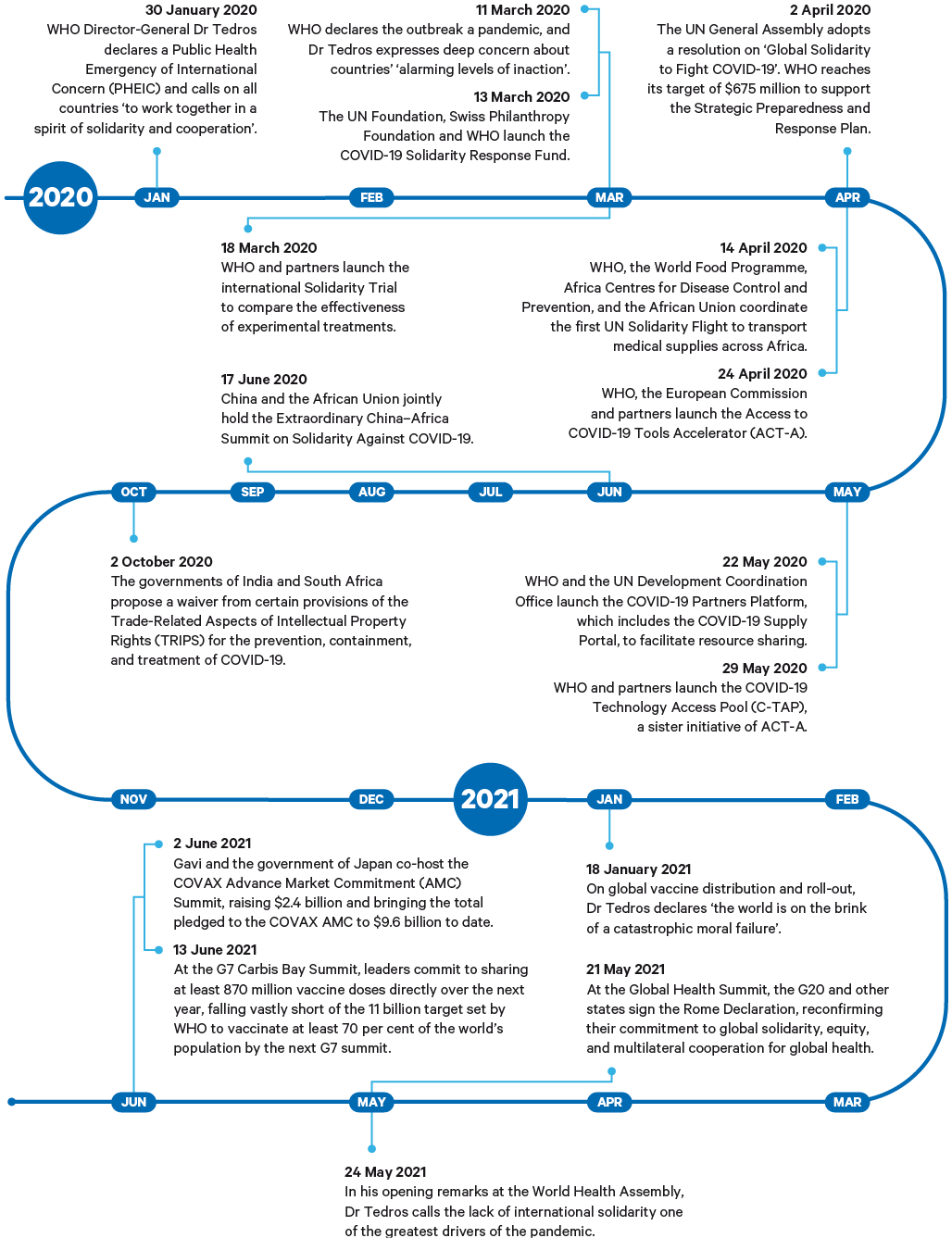
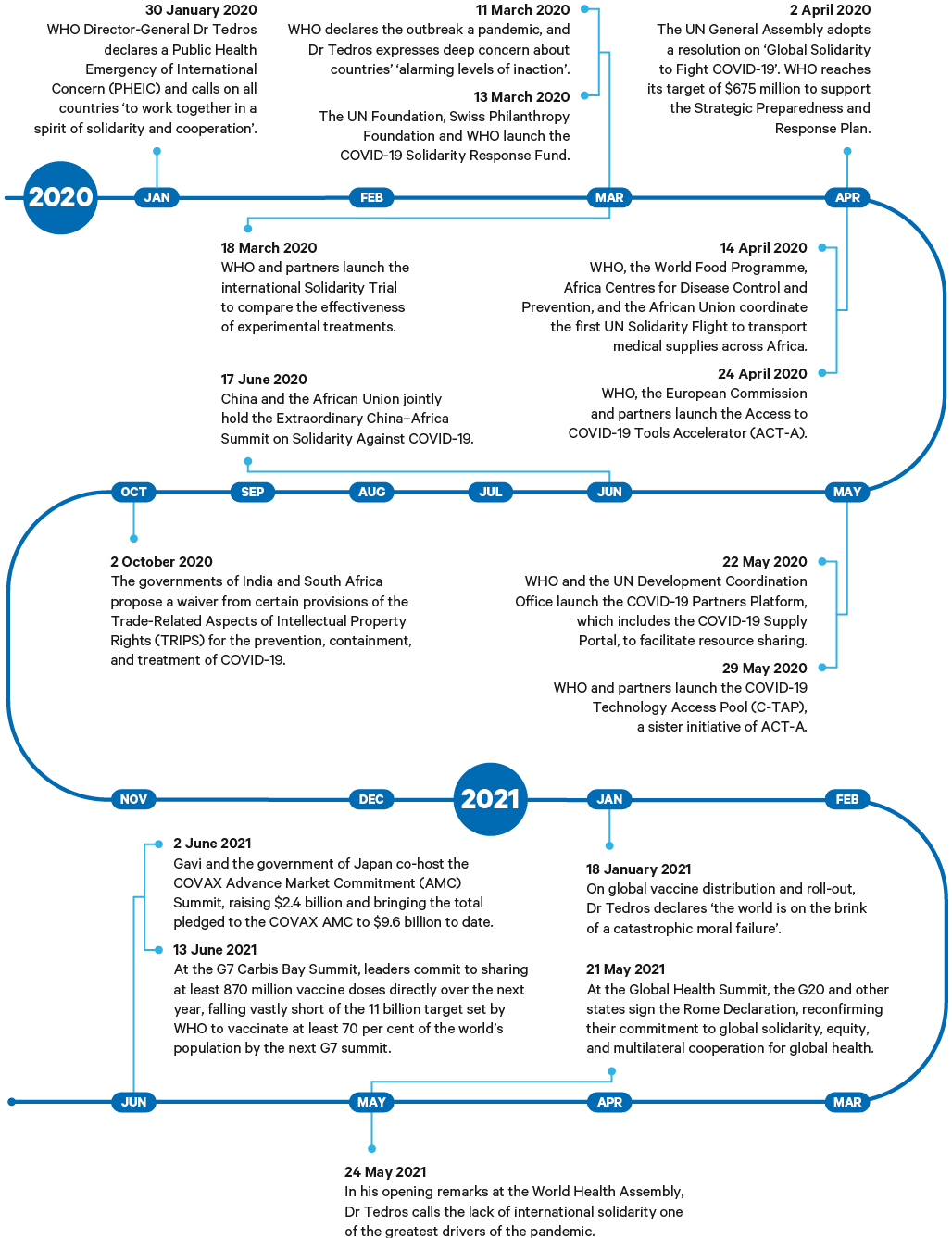
Source: Gavi (2021), ‘Key Outcomes: COVAX AMC 2021’, 10 May, https://www.gavi.org/sites/default/files/covid/covax/COVAX-AMC-Donors-Table.pdf (accessed 25 Jun. 2021).
By mid-July 2021, COVAX had delivered over 100 million doses to 135 countries. This leaves it far short of its target of 2 billion doses for 2021, mainly because COVAX deliveries have been severely disrupted as a result of the vaccine export ban introduced by India in March 2021 as its domestic cases surged dramatically.
Most interviewees thought that ACT-A and COVAX had introduced a new dynamic in the global discussion, bringing together in one forum not just governments but also key international and philanthropic organizations and stakeholders including the private sector. These were considered important innovations, notably in building in concerns about global equity and access from the beginning, rather than as an afterthought. As one interviewee put it:
But some also questioned the development aid model underlying ACT-A. Interviewees acknowledged the limitations of this paradigm, and the present impact on countries’ collective ability to engage meaningfully in solidarity-based approaches. As one pointed out:
There is a group of ‘usual suspect’ donor governments and philanthropic bodies with a focus on global health that set the framework for initiatives like COVAX without adequately consulting all stakeholders, particularly those in LMICs. But the pandemic has overturned the assumption that richer countries are necessarily better prepared and better equipped to support collective efforts. Instead, it has exposed gaps in public health intelligence and infrastructure in many HICs – which, as one interviewee remarked, ‘is ironic because that’s what Europe and North America try to teach the world’ (ML-036). Many interviewees recognized the pandemic as representing a pivotal shift in power relations and hierarchies within the current global health paradigm, and an opportunity for solidarity to truly manifest mutual assistance and support between countries.
Rather than equating solidarity with a financial transaction between countries, several interviewees encouraged other, more sustainable forms of bilateral solidarity, such as technical assistance and training, data and information sharing, exchanging experiences and best practice, and technology transfers – activities currently missing from the global solidarity toolbox.
The issues concerning COVAX, vaccines and solidarity are further examined
in Chapter 3.
Access to critical resources
The pandemic has revealed major vulnerabilities in the global supply chain and distribution infrastructure for medical supplies and equipment. Despite multilateral efforts to coordinate the logistics of supply and demand, for example by increasing purchasing power, procuring and protecting scarce resources, and establishing air traffic to deliver procured goods, countries have engaged in various actions that are deleterious to solidarity. These have included hoarding scarce resources, price gouging, cornering early supplies, hijacking global supply chains and controlling distribution unfairly. Hence, while most countries had the financial means to procure resources, many lacked the physical and material access to the pool of resources. As one interviewee said:
In the initial stages of the pandemic, many countries reacted to the shortage of PPE when faced with rapidly rising hospital admissions by unilaterally banning exports of such items, while also taking measures to liberalize imports. The EU reacted to unilateral export bans by some member states by imposing EU-level authorizations for PPE exports in March 2020. Similarly, the US introduced extensive restrictions in April 2020. In that same month, the World Trade Organization (WTO) recorded that 80 countries had introduced export restrictions. The directors-general of the WTO and WHO issued a joint statement on 20 April 2020:
In many countries these restrictions were subsequently relaxed – for example, the EU measures were allowed to expire on 26 May 2020 – but in others the measures continued. In January 2021 the US extended restrictions on several PPE exports until 30 June 2021, but these were not then further renewed.
One researcher from Latin America interviewed in November 2020 needed PPE for a research project with US collaborators:
Export restrictions are a prime example of putting one’s own country first and failing to demonstrate solidarity with other countries. Apart from obviously affecting countries that were previously importers, production systems depend on international supply chains that are disrupted by export controls, not to mention the likelihood of beggar-thy-neighbour retaliation. Restricting the exports of raw materials required to manufacture PPE (e.g. textiles) threatens production in third countries. Thus export restrictions can fuel shortages. Nevertheless, the EU once again resorted to temporary export authorizations when faced with shortfalls in its vaccine deliveries in January 2021. It required EU member states to submit to the EU Commission proposed export authorizations, and to decide on the request in accordance with the Commission’s opinion. As already noted, in March 2021 India, the largest supplier of vaccines for COVAX recipients, imposed a ban of unspecified duration on vaccine exports. Vaccine producers have also raised concerns about the possibility of export restrictions affecting their access to needed inputs. These include the implications of the use of the Defense Production Act in the US to secure inputs for US producers to the possible detriment of producers elsewhere.
Solidarity in science
Science, in all its different disciplines, has been central to the fight against the pandemic. Sharing the fruits of scientific endeavour as widely and as rapidly as possible is critical in a fast-moving pandemic where speed is of the essence. Scientists around the world have shown solidarity in generating an unprecedented level of research publications – more than 450,000 research publications related to COVID-19 were recorded by May 2021. Moreover, there has been a push for wider and more timely access. Major scientific journals (and news outlets) have shown solidarity by removing articles on COVID-19 from paywalls for the duration of the pandemic, and have significantly reduced the time from submission to publication. There has also been a flourishing of preprints, articles published in a large number of repositories such as bioRxiv and medRxiv, as first drafts before peer review. This has meant that scientific results of consequence for response policies have been disseminated much earlier than would normally be the case.
The solidarity expressed through the widespread international sharing of genomic sequences has been beneficial to the pandemic response in a number of ways. The Global initiative on sharing all influenza data (GISAID) was established in 2008 for the rapid sharing of data on influenza viruses, but is now the main global repository for coronavirus sequences. The platform fosters collaboration among researchers worldwide. By July 2021 it had posted more than 2 million full genome sequences from all over the world. WHO’s Chief Scientist, Dr Soumya Swaminathan, has described it as a game-changer. The global sharing of gene sequences is an excellent example of scientific collaboration and open sharing that has allowed scientists and policymakers to generate appropriate responses in real time. For example, vaccine producers are able to work immediately on adjusting their vaccines to make them effective against new variants.
The global sharing of gene sequences is an excellent example of scientific collaboration and open sharing that has allowed scientists and policymakers to generate appropriate responses in real time.
Much of this enhanced sharing of research occurred spontaneously, reflecting the actions of researchers and publishers. But WHO has also played a wider role in seeking to accelerate and coordinate the activities of researchers around the world to focus on the priorities of combating the current pandemic and preparedness planning for future epidemics. Building on the scientific collaboration platforms it initiated during the 2003 SARS epidemic, WHO has fostered solidarity among scientists by convening meetings to discuss appropriate responses to the pandemic. For example, in February 2020 it organized a meeting of approximately 400 researchers from around the world to contribute to building a Global Research Roadmap. In January 2021 it convened meetings of scientists to identify knowledge gaps and set research priorities for vaccines against the virus, and to expand scientific collaboration in the monitoring of emerging variants of SARS-CoV-2. These meetings included, respectively, more than 2,800 scientists from 130 countries, and 1,750 experts from 124 countries.
In addition, in March 2020 WHO launched the ‘Solidarity’ clinical trials. This was in response to its concerns about the fragmented approach to the science: a large number of small trials with different methodologies were being undertaken around the world that failed to generate adequate evidence to demonstrate effectiveness. The first ‘Solidarity’ trial was one of the largest international randomized trials for COVID-19 treatments, enrolling almost 12,000 patients in 500 hospital sites across 30 countries. The first results, announced in October 2020, demonstrated that all four treatments the trial evaluated had little or no effect on patients, including a therapy promoted by the then US president.
While collaboration is an important aspect of demonstrating international solidarity, national efforts can demonstrate solidarity by making new knowledge available to the world as a global public good. For example, in June 2020 the RECOVERY trial in the UK found the first effective treatment for COVID-19 – dexamethasone. In February 2021 it found that adding the monoclonal antibody tocilizumab reduced mortality by up to one half. The results from both studies can be immediately applied in treatment protocols throughout the world. Similarly, knowledge gained from the experience of specific countries and shared with the world, such as Iceland’s and Japan’s insights into ‘superspreading’ events, and Japan’s demonstration that a ‘cluster-busting’ approach – which focused on preventing a cluster of infections linked to a single event from progressing to generalized community transmission by identifying clusters and targeting contact tracing and testing resources at them – was effective in controlling outbreaks, rapidly informed responses in the rest of the world.
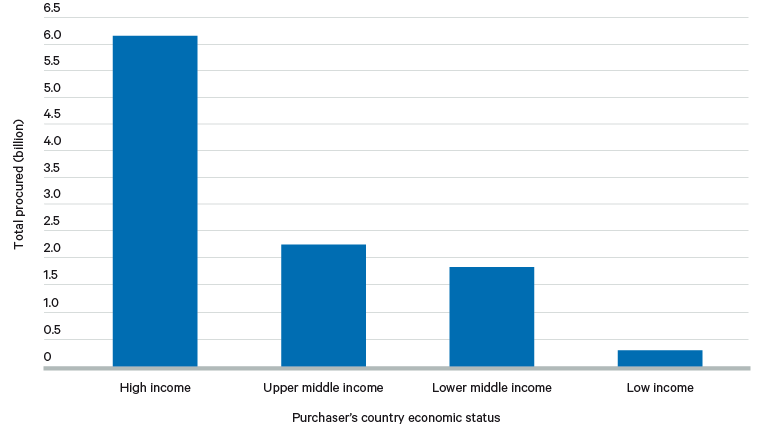
Another example of national effort conferring global benefit is the investments that high-income governments and others made in vaccine development in order to secure doses for their own populations. This has rightly led to criticisms about ‘vaccine nationalism’. Yet, paradoxically, it is these investments, motivated principally by self-interest, that have enabled a number of effective vaccines to be developed and authorized in record time. Without them, the rest of the world would not have had potential access to the range of vaccines now becoming available. Figure 2 shows the distribution of vaccine purchases by country income level.