|
|
|
|
|
|
|---|
|
Mar. 2011–
|
PHR
|
PHR
|
All Syria – Global coverage
|
Secondary
|
|
Jun. 2011–
|
VDC
|
Violations Documentation Center
|
All Syria
|
Primary
|
|
Jun. 2011– (AHCC: Nov. 2016–)
|
SNHR
|
Syrian Network for Human Rights
|
All Syria
|
Primary
|
|
Feb. 2014–
|
SAMS
|
SAMS
|
Opposition- controlled areas
|
Primary
|
|
Apr. 2015–
|
SiND
|
Insecurity Insights
|
All Syria – Global database
|
Secondary
|
|
2015–17
|
Annual reporting
|
Safeguarding Health in Conflict
|
All Syria – Global database
|
Secondary/ Primary
|
|
Nov. 2015–Mar. 2018
|
MVH
|
WHO-led Health Cluster in Gaziantep, Turkey
|
Opposition- controlled areas
|
Primary
|
|
Mar. 2018–
|
SSA
|
WHO
|
All Syria
|
Primary and secondary
|
|
Not known
|
HCiD
|
ICRC
|
Syrian government- controlled areas
|
Primary
|
|
Not known
|
MRM
|
UNICEF
|
All Syria and Syrian government focus
|
Secondary
|
Three principal types of actor are involved in reporting AHCC in Syria: humanitarian health responders; human rights agencies; and legal actors. Data practices – i.e. the collection, verification and use of data – reflected the objectives and purpose of the governing agency. While reporting by health actors tends to be more representative and extensive in documenting all alleged incidents, reporting by legal actors used more rigorous, case-by-case approaches to establish proof and intentionality and to identify perpetrators. While many human rights organizations had general reporting on human rights violations, some, such as the Syrian Network for Human Rights (SNHR), created a special reporting tool for AHCC.
PHR’s reporting played a key role in bringing global attention to the issue of attacks on healthcare facilities, and encouraged local and international health actors to engage in reporting such attacks.
The first organization to report on AHCC in a systematic way was PHR, which did so from the onset of the conflict in April 2011. PHR’s reporting played a key role in bringing global attention to the issue of attacks on healthcare facilities, and encouraged local and international health actors to engage in reporting such attacks. In the first three years of the conflict, AHCC incidents were reported as human rights violations or IHL infractions by local organizations, such as the Violations Documentation Center (VDC) and the SNHR. From 2013, PHR began building the capacity of local health and human rights actors to help expand and improve the reporting and documentation of AHCC. SAMS, which established its reporting mechanism in 2014, was considered the leading local medical actor in reporting AHCC. The Syrian health directorates also played a key role in documenting and archiving AHCC incidents in each governorate and supported the health cluster efforts. While a wide range of agencies and organizations participated in the collection and publication of data on AHCC, efforts were not made to establish an overarching dataset combining all reports.
An analysis was conducted of the methodologies used across the above-mentioned mechanisms, in order to assess which held most relevance for comparative study. Five mechanisms emerged as the best candidates. The prioritization was performed by means of an unstructured process, based on numerous factors: these included specificity both to the context and to AHCC, wide geographical coverage, representativeness, completeness and the strictness of verification processes. The five mechanisms thus identified for further comparative study were:
- MVH
- PHR
- SAMS reporting
- SiND
- SNHR reporting
A comparison of AHCC reporting mechanisms in Syria
A comparison was conducted using governorate-level monthly data from the mechanisms listed above. All datasets were publicly available with the exception of the SAMS dataset, which was obtained through a data-sharing agreement. The data then were cleaned and merged within a single set. A basic descriptive analysis was conducted, followed by a multivariate test to establish continuity and discrepancies between the constituent datasets. Due to the heterogeneity of these datasets, statistical approaches have been accompanied by a visual presentation of the study’s findings for the sake of clarity and comparison. The software used for the quantitative analysis was Stata 15.
Table 2 summarizes the main descriptive analysis. By running a multivariate test on the means, some weak evidence emerged to suggest that the data varied between different mechanisms (P value = 0.0663). This difference could be attributed to various factors. These factors will be discussed in the following sections.
|
|
|
|
|
|
|
|
|---|
|
Mar. 2011–Dec. 2017
|
PHR
|
81
|
492
|
0–16
|
6.01
|
0–15
|
|
Feb. 2014–Dec. 2017
|
SAMS
|
48
|
463
|
0–41
|
9.65
|
0–27
|
|
Apr. 2015–Oct. 2017
|
SiND
|
31
|
434
|
0–51
|
14
|
1–33
|
|
Jan. 2016–Dec. 2017
|
MVH
|
24
|
267
|
0–30
|
11.29
|
3–22
|
|
Nov. 2016–Dec. 2017
|
SNHR
|
15
|
377
|
6–56
|
25.13
|
11–43
|
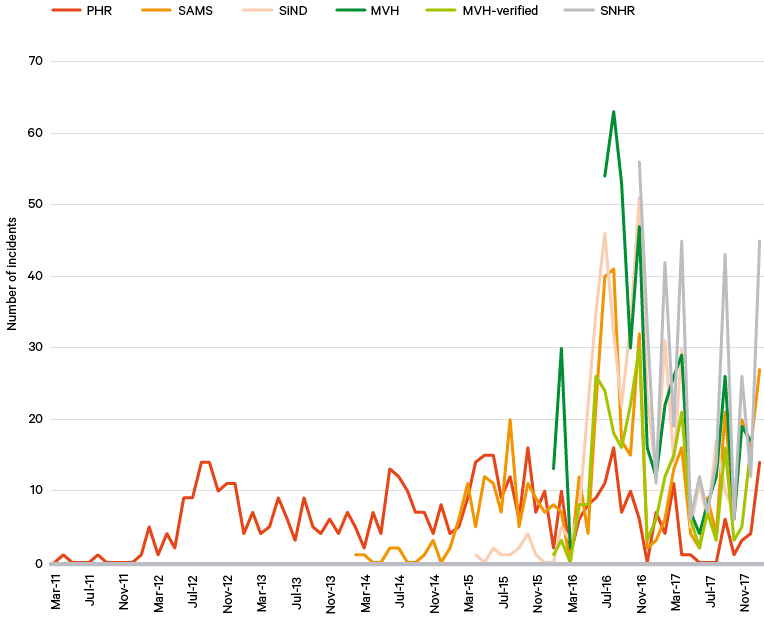
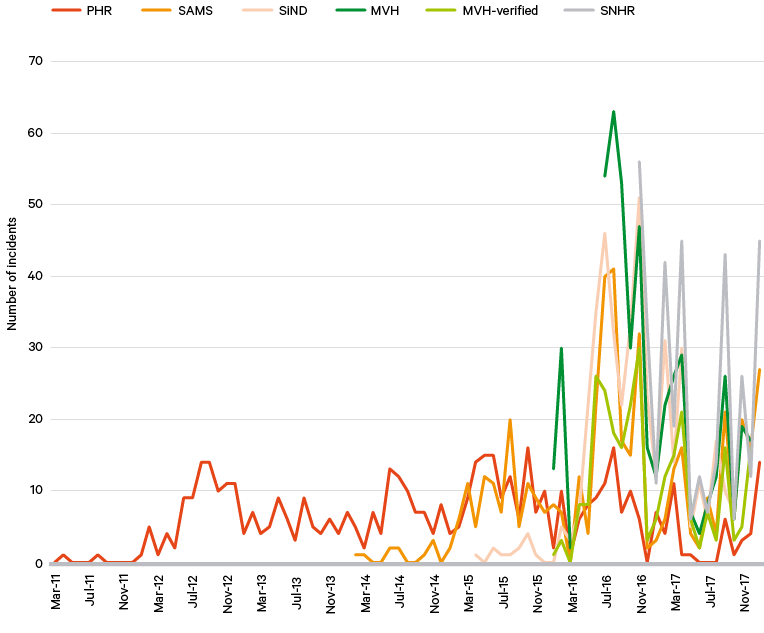
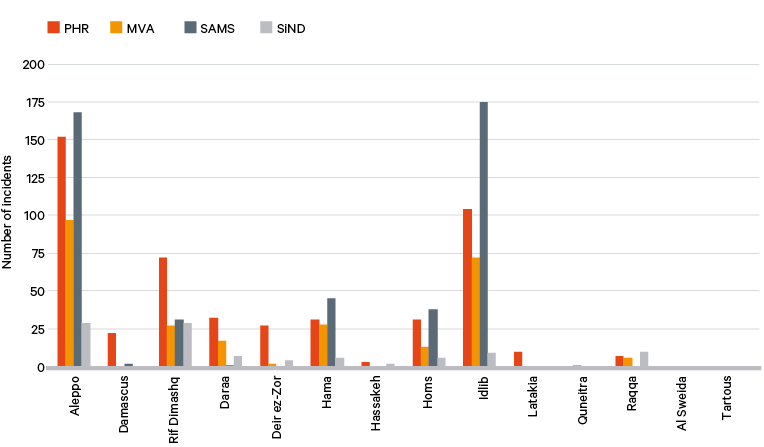
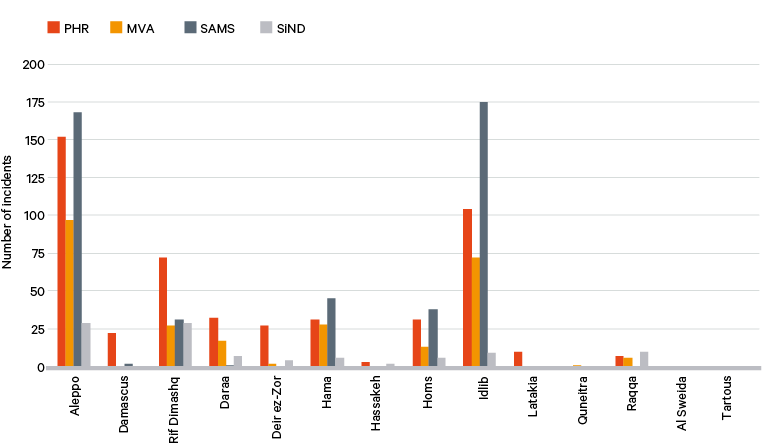
Despite the differences between these reporting mechanisms, there remains an approximate symmetry across them. As Figure 1 shows, all mechanisms indicate synchronized peaks of AHCC incidents, especially during military events that have attracted wide media attention such as the invasion of the eastern section of Aleppo city by Syrian government forces in 2016. Also, the periods with minimum incidents tend to be concurrent across all mechanisms, synchronized with the implementation of cessation of hostilities agreements, for example in March 2016 and the summer of 2017. A study published by the open-access journal PLOS Medicine in 2018 compared individual incidents of AHCC in Syria as documented in two reporting mechanisms (SAMS and PHR) and found that there was some overlap. Mechanisms that use primary data sources tend to capture more incidents than those that rely solely on secondary sources. This suggests that secondary data, such as media reports, miss a proportion of AHCC incidents.