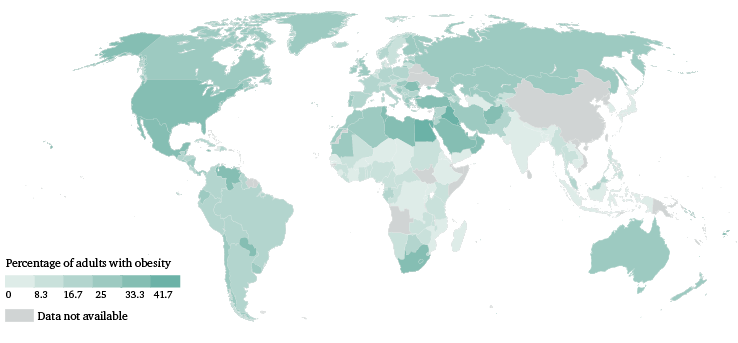
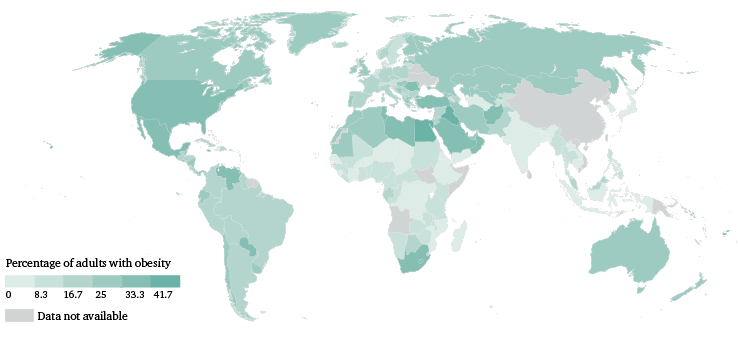
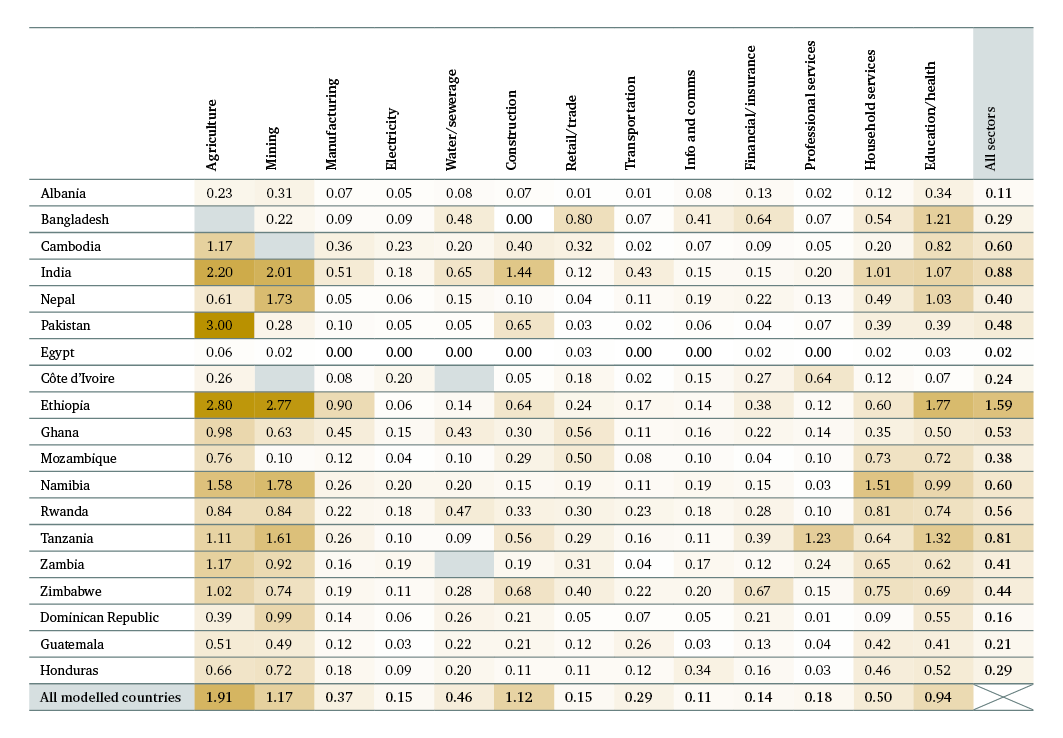
In fact, our model shows that sectors characterized by physically demanding roles suffer the greatest costs associated with obesity among the workforce: across the 19 countries modelled, the cost of obesity is most concentrated in mining, education and health, and household services. In Egypt and Albania, where the prevalence of workforce obesity is particularly high, it is the agricultural sector that experiences the greatest costs. The economic burden of obesity on businesses is highest in Egypt, Albania and Honduras (Figure 9), countries where obesity is highly prevalent across the workforce (Annex II – Figure 18) and across the population as a whole (Figure 6). In these countries, and also in the Dominican Republic, Guatemala, Ghana, Namibia and Zimbabwe, the costs of workforce obesity exceed those of workforce underweight (Figures 7 and 9).
2.2 The additional costs of anaemia and childhood stunting
2.2.1 Anaemia among the workforce
Anaemia, as one example among many types of micronutrient deficiency, reduces the physical capacity of workers, particularly those engaged in manual labour (Annex I – Table 7). As with workforce underweight, workforce anaemia is particularly costly to the agriculture and mining sectors, costing them 3 per cent of GVA and 1.1 per cent of GVA respectively across the five countries modelled (Albania, Ethiopia, India, Namibia and Zimbabwe). Generally speaking, a lower prevalence of manual workers with anaemia corresponds with a lower relative cost per sector, but two sectors buck this trend: mining, and education and health. Despite a relatively low prevalence of manual workers with anaemia, both sectors have a high proportional GVA loss. This is likely a reflection of the fact that output in both sectors is much more reliant on human capital – worker productivity – than on technology or equipment, meaning that losses to productive capacity among the workforce have a more direct impact on economic performance.
Women workers are 1.4 to 2.6 times more likely to be anaemic than their male counterparts
Women in the workforce are much more likely than men to be anaemic (though prevalence among women in the workforce is slightly lower than among the female population as a whole). Women workers are 1.4 to 2.6 times more likely to be anaemic than their male counterparts, and this holds true even within occupation categories: 30 per cent of women in skilled agriculture and elementary occupations are anaemic, compared with 17 and 23 per cent of their male counterparts respectively (Annex II – Figure 22). Anaemia reduces economic output by an additional 0.8 per cent of GDP on average. Anaemia costs India alone $20 billion (0.7 per cent of GDP) in lost worker productivity. Given that anaemia arises from a single mineral deficiency, the actual impacts and costs of micronutrient deficiencies on the economics of business are likely to be significantly under-represented by our analysis.
2.2.2 Experience of childhood stunting among the workforce
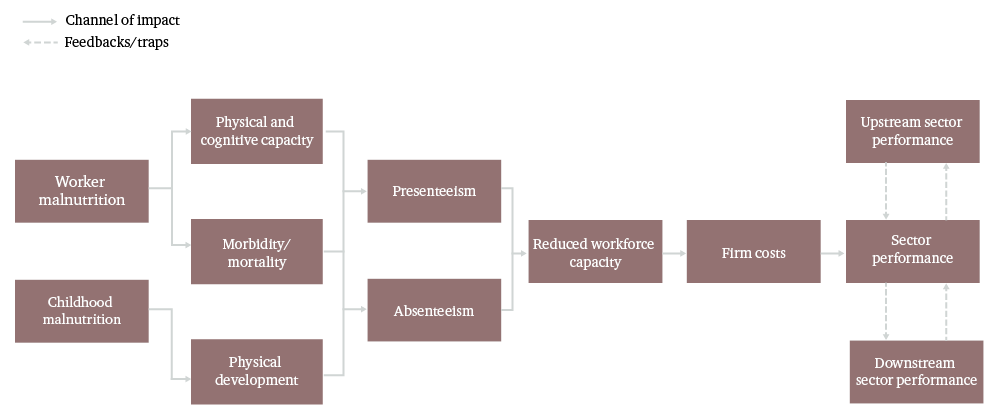
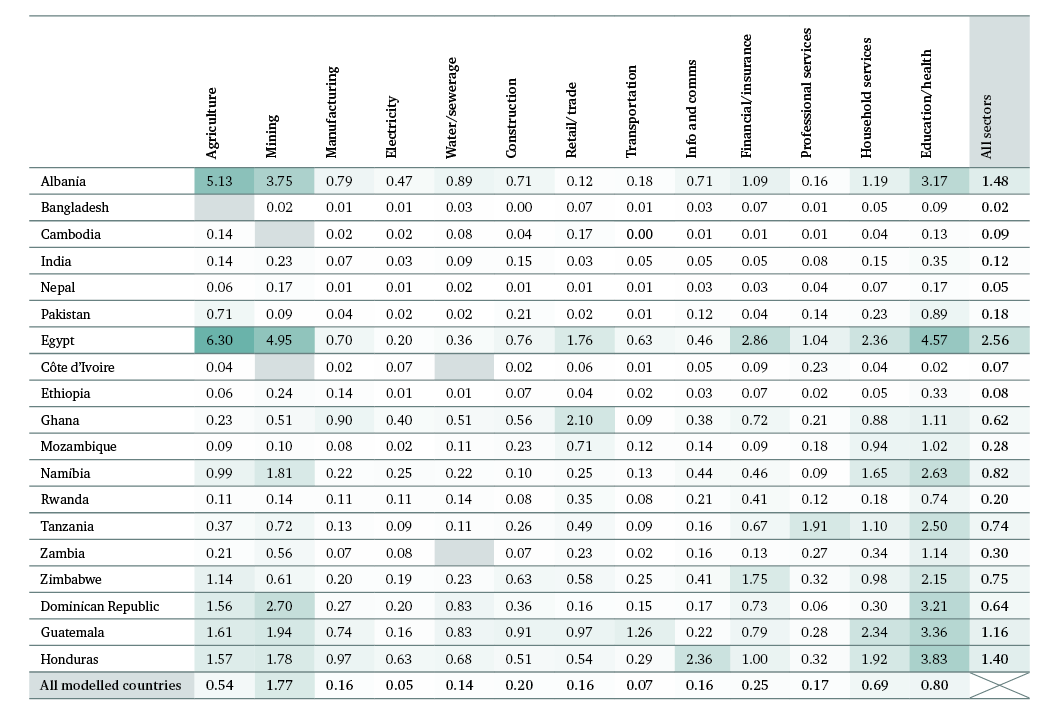
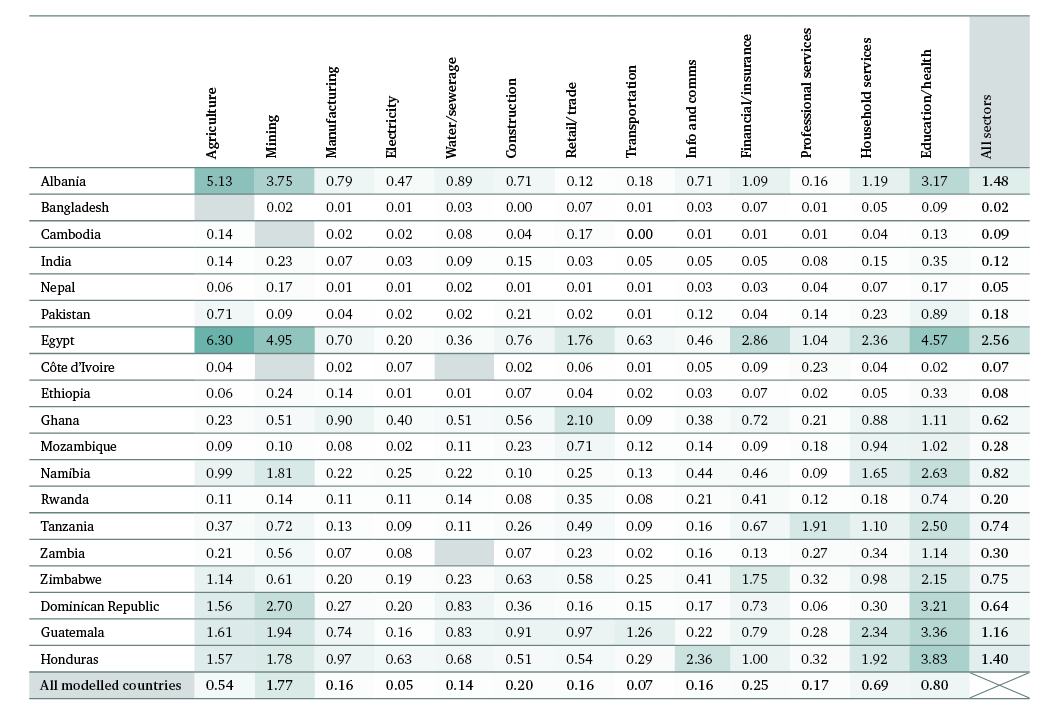
We undertook a partial exploration of the effects of stunting experienced in childhood on adult workers and their labour productivity, using adult short stature as a crude proxy for the physical impacts of childhood stunting. Data on adult short stature were available for only 17 of the 19 countries (Côte d’Ivoire and India are not included). Across the 17 countries, just under a sixth of the workforce (16 per cent) is estimated to be suffering the physical effects of childhood stunting. The prevalence of adult short stature among the current workforce is particularly high in Central America (with rates of 60 per cent in Guatemala and 30 per cent in Honduras) and Southeast and South Asia (with rates of 27 per cent in Cambodia and 26 per cent in Pakistan).
Across the 17 countries for which data on prevalence were available, the physical impacts of childhood stunting are estimated to impose a cost to business of $3.9 billion annually, equivalent to 0.4 per cent of GDP. This is likely to be a significant underestimate of the true total, as stunting also reduces cognitive development and educational attainment. Were the indirect impacts of childhood stunting on educational attainment to be included, a first-pass calculation suggests the costs could increase by 4.5 times, up to a total of 1.8 per cent of GDP (Annex I – Box 11). Moreover, it is likely that the impacts of childhood stunting are even more significant for economic development. The cognitive and educational impacts of childhood malnutrition are likely to have a dynamic effect on the economy, such as the value of the labour force, the education status of the labour force and the size of economic sectors. Further research is needed to examine this effect and quantify the likely impact on business.
Despite the significant and long-term impacts of childhood stunting on labour productivity, only one of the 19 interview participants noted that the company’s workers in low- and middle-income countries would likely have been affected by stunting in childhood.