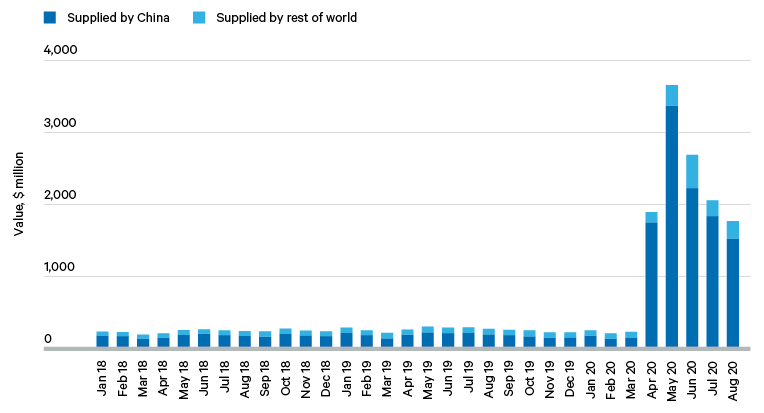
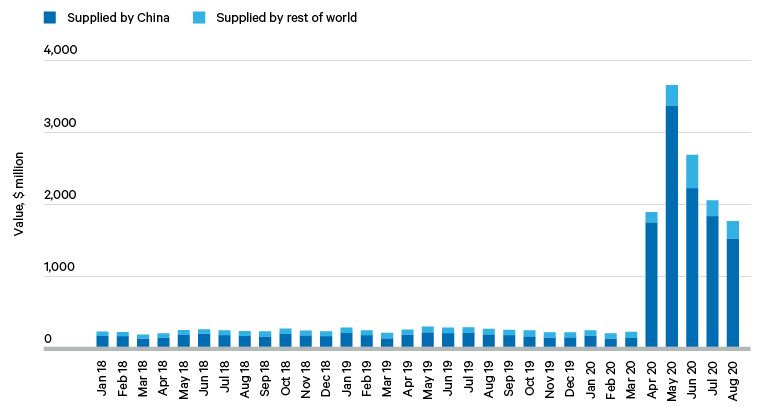
The proposed diversification of supply has also come under increased scrutiny. During the past nine months, evidence has come to light casting doubt on claims that the sourcing of medical goods was concentrated in too few foreign nations to ensure reliable supply. Careful parsing of data on imports of individual medical products reveals that, contrary to common belief, China is the majority supplier of only a tiny fraction of the categories of medical goods imported by France, Germany, the UK and the US. A similar analysis of data for the entire EU confirms little ‘overdependence’ on imports from China. For the US, once domestic production is taken into account, China’s share of the US domestic medical equipment market was only around 8 per cent before the pandemic hit. As such, the rhetorical tactic of critics of cross-border supply chains – in highlighting what they think are telling examples of supply vulnerabilities – has been shown to be unrepresentative of realities on the ground and, therefore, an unsound basis for public policy.
Once the literature on supply chain management is consulted, the weaknesses become apparent in the broad-brush policy recommendations advanced last year to repatriate or reshore production or diversify suppliers. First, there is considerable diversity across the supply chains used to manufacture different types of medical equipment (such as ventilators), medical consumables (such as PPE) and medicines. Policy initiatives need to be tailored to the specificities of each supply chain.
Second, many politicians and commentators have appropriated the terms used to describe firm-based strategies for managing disruption in cross-border supply chains, and have applied these apparently with little thought to the national level. But what may be appropriate for individual companies does not automatically translate to the national context. A given firm’s supply chain may be ‘resilient’ (however defined) in isolation, but a government needs to concern itself with whether, taken together, all of the suppliers of a particular type of medical product are resilient.
There is the potential here for a classic fallacy of composition. If every firm took identical resilience measures, it might expose a national health system to significant location-specific risks. Governments have to think differently from firms about managing sector-wide supply chain disruption. This means that stress tests performed by governments need to be different from those undertaken by, or applied to, any one firm.
Third, even some of the seemingly unobjectionable policy recommendations put forward in the past year wilt under scrutiny. Take the recommendation that a firm diversify its sourcing across multiple locations. This may indeed have the intended effect of reducing the probability of the firm failing to deliver to its customers should any one supplier be unable to meet its commitments. However, maintaining multiple suppliers, or suppliers across multiple locations, incurs additional costs and brings risks of its own (see Table 1).
Moreover, as a comprehensive recent study of steps by thousands of firms to manage their international supply chains shows, the time needed to restore operations after a disruption is longer for firms with more diversified sourcing. While diversification reduces the risk of disruption, this is at the expense of prompt restoration of operations should such disruption occur. This evidence implies that there are always trade-offs when it comes to reducing supply risks.
From the perspective of managing cross-border supply chain disruptions, business experience has also revealed that there are pros and cons in developing long-term relationships with suppliers. The same applies to sourcing from locations with better logistics infrastructure, even though such suppliers may in principle be able to facilitate faster shipment in response to changing demand (see Table 1).
Overall, many official statements about the deficiencies of cross-border supply chains, and how to fix them, bear little relation to the evidence from sourcing patterns on the ground. Nor have such statements accurately reflected the diversity of supply chains among firms even within the same broad sector of medical goods, or the ways in which firms have lessened disruption-related risks in their cross-border supply chains.